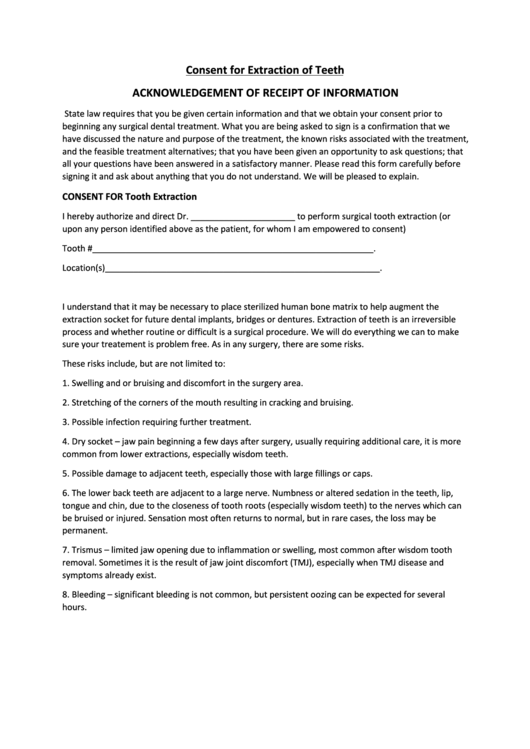
Consent Form For Extraction - This form and your discussion with your doctor are intended to help you make informed decisions about your surgery. _____ date of birth_____ first last it has been recommended that i have. As a member of the. Informed consent for tooth extractions & oral surgery patient’s name: As a member of the. This form and your discussion with your doctor are intended to help you make informed decisions about your surgery.
As a member of the. This form and your discussion with your doctor are intended to help you make informed decisions about your surgery. Informed consent for tooth extractions & oral surgery patient’s name: _____ date of birth_____ first last it has been recommended that i have. As a member of the. This form and your discussion with your doctor are intended to help you make informed decisions about your surgery.
This form and your discussion with your doctor are intended to help you make informed decisions about your surgery. This form and your discussion with your doctor are intended to help you make informed decisions about your surgery. _____ date of birth_____ first last it has been recommended that i have. As a member of the. As a member of the. Informed consent for tooth extractions & oral surgery patient’s name:
Printable Dental Extraction Consent Form Printable Forms Free Online
Informed consent for tooth extractions & oral surgery patient’s name: This form and your discussion with your doctor are intended to help you make informed decisions about your surgery. As a member of the. As a member of the. This form and your discussion with your doctor are intended to help you make informed decisions about your surgery.
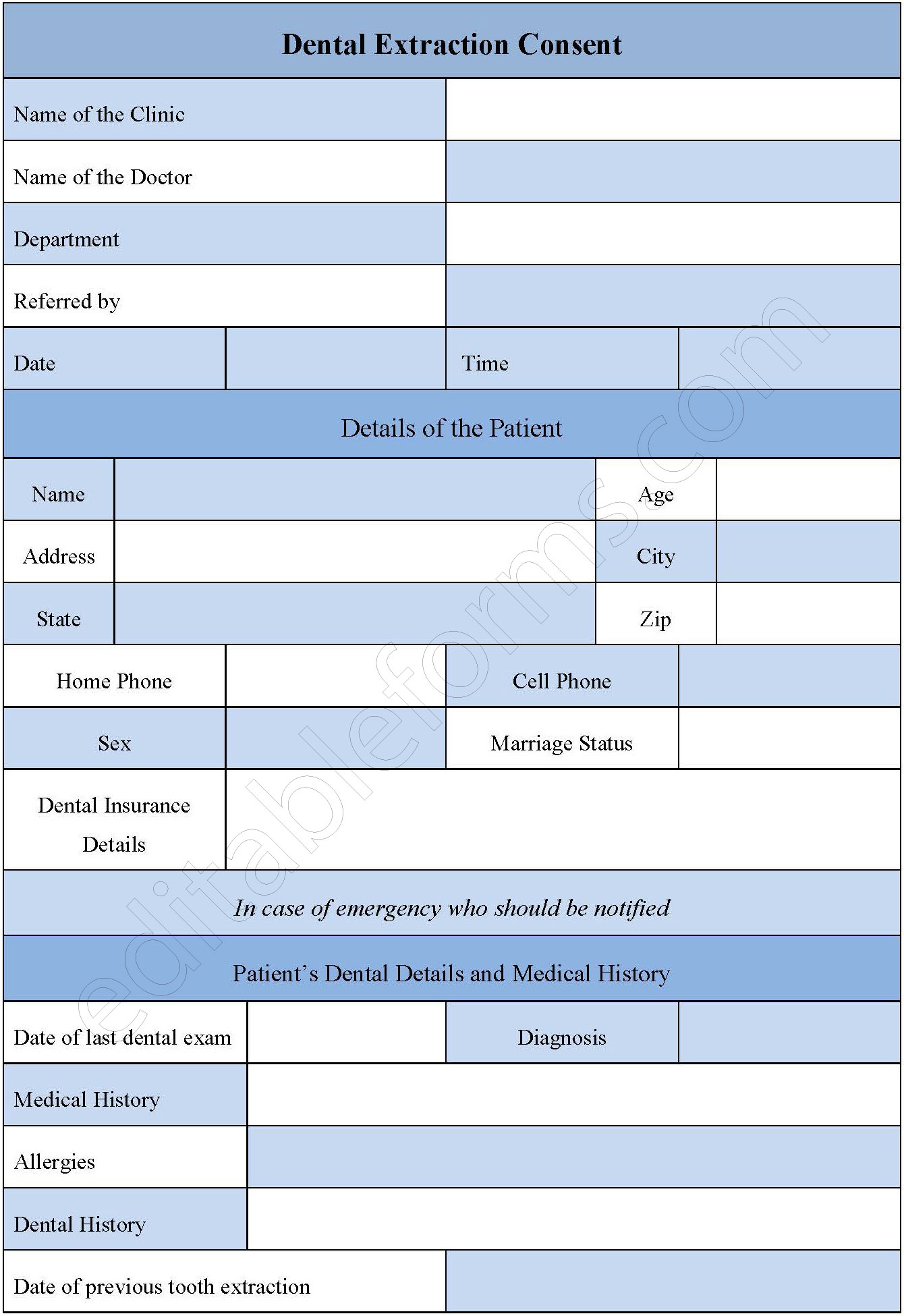
Dental Extraction Consent Form Editable PDF Forms
As a member of the. As a member of the. This form and your discussion with your doctor are intended to help you make informed decisions about your surgery. Informed consent for tooth extractions & oral surgery patient’s name: This form and your discussion with your doctor are intended to help you make informed decisions about your surgery.
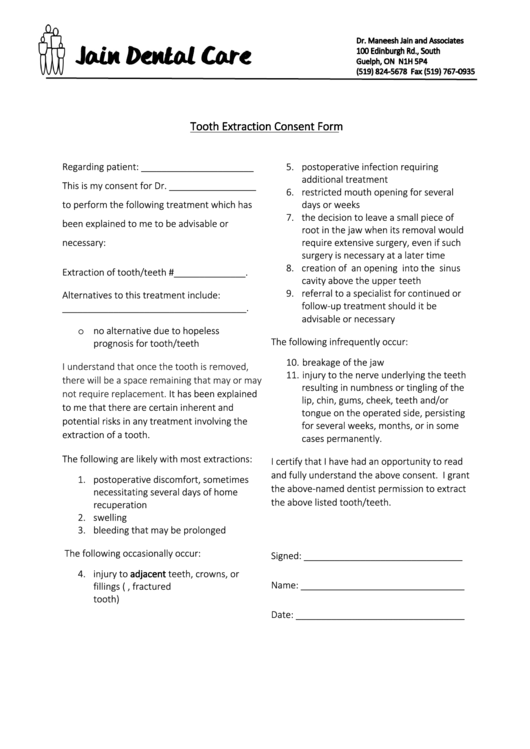
Extraction Consent Form Dental 2022
As a member of the. This form and your discussion with your doctor are intended to help you make informed decisions about your surgery. As a member of the. This form and your discussion with your doctor are intended to help you make informed decisions about your surgery. Informed consent for tooth extractions & oral surgery patient’s name:
Dental Extraction Consent Form Printable Consent Form
Informed consent for tooth extractions & oral surgery patient’s name: _____ date of birth_____ first last it has been recommended that i have. As a member of the. This form and your discussion with your doctor are intended to help you make informed decisions about your surgery. As a member of the.

CONSENT FORM FOR SURGICAL TOOTH EXTRACTIONS AND
_____ date of birth_____ first last it has been recommended that i have. As a member of the. Informed consent for tooth extractions & oral surgery patient’s name: As a member of the. This form and your discussion with your doctor are intended to help you make informed decisions about your surgery.

Dental Extraction Consent Form Editable PDF Forms
As a member of the. As a member of the. This form and your discussion with your doctor are intended to help you make informed decisions about your surgery. _____ date of birth_____ first last it has been recommended that i have. This form and your discussion with your doctor are intended to help you make informed decisions about your.
Printable Dental Extraction Consent Form
As a member of the. This form and your discussion with your doctor are intended to help you make informed decisions about your surgery. As a member of the. _____ date of birth_____ first last it has been recommended that i have. This form and your discussion with your doctor are intended to help you make informed decisions about your.

Extraction Consent
This form and your discussion with your doctor are intended to help you make informed decisions about your surgery. As a member of the. _____ date of birth_____ first last it has been recommended that i have. This form and your discussion with your doctor are intended to help you make informed decisions about your surgery. Informed consent for tooth.

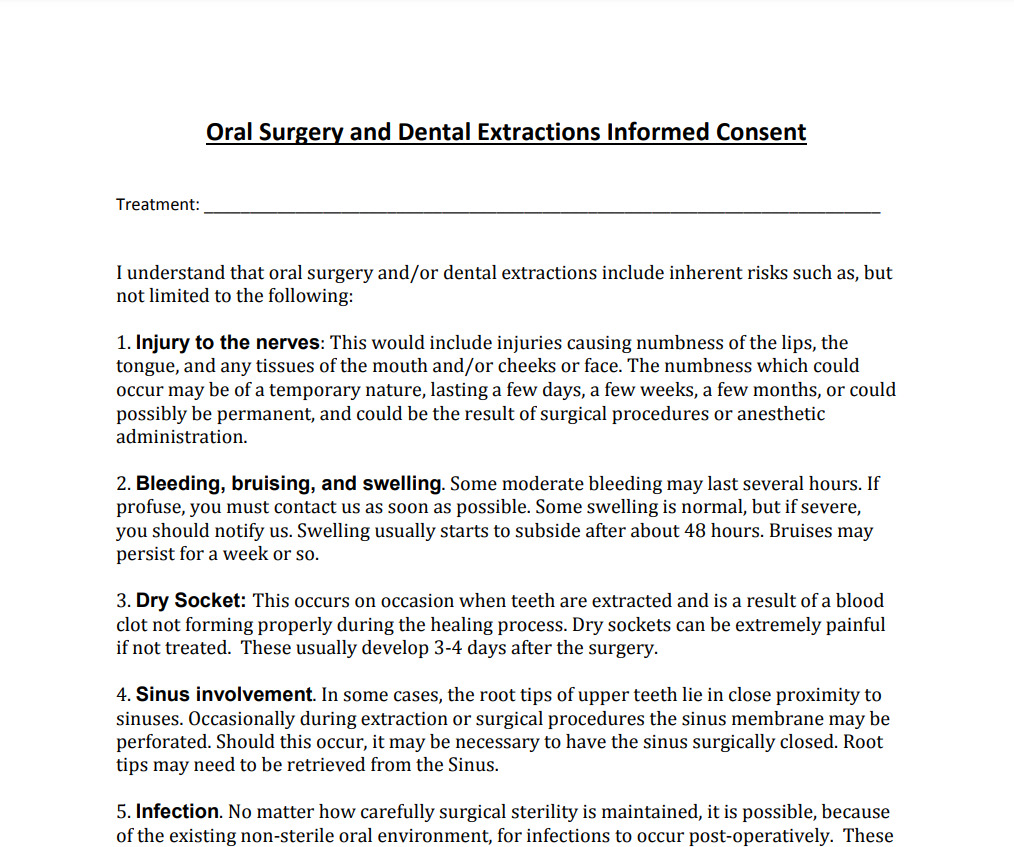
Extraction Informed Consent, Extraction Consent Form, Extractionl Form
As a member of the. This form and your discussion with your doctor are intended to help you make informed decisions about your surgery. Informed consent for tooth extractions & oral surgery patient’s name: _____ date of birth_____ first last it has been recommended that i have. This form and your discussion with your doctor are intended to help you.
Dental Extraction Consent Form Editable PDF Forms
This form and your discussion with your doctor are intended to help you make informed decisions about your surgery. As a member of the. As a member of the. Informed consent for tooth extractions & oral surgery patient’s name: This form and your discussion with your doctor are intended to help you make informed decisions about your surgery.
This Form And Your Discussion With Your Doctor Are Intended To Help You Make Informed Decisions About Your Surgery.
As a member of the. As a member of the. This form and your discussion with your doctor are intended to help you make informed decisions about your surgery. Informed consent for tooth extractions & oral surgery patient’s name: